Featured Slider
Category:

In Uganda safe spaces, toll free line offers SRHR information for young people
Uganda – “We’ve been told that our clinics bear peace – the clinic and what is offered in it,” said Demeter Margaret Namuyobo. She is the Medical Coordinator at Reproductive Health Uganda (RHU), where we present a safe space for women and young people in Uganda, to access sexual reproductive health services and information (SRHI).
Over the past 65 years, millions of marginalized and underserved people have entered Uganda, including internally displaced persons (IDPs), refugees, young people, and migrants fleeing economic and political instability in Sudan, South Sudan, Ethiopia, Somalia, the Democratic Republic of the Congo (DRC), Burundi, and Rwanda.
New Patient care Centres in all 19 static RHU clinics and a toll-free line (0800299003), assist new arrivals in gaining access to SRHI services and information, as well as addressing urgent needs such as protection, shelter, food, and counseling.
Amid the noise, crowds, and queues at community outreaches and the static clinics, there is a door marked with the words
“This is the RHU safe space” – a place where young people and survivors of gender-based violence can come for guidance, care, and referrals to local networks of public services as well as resources on sexual and reproductive health.
“The people who come here have SRHI issues that require urgent attention, in most cases privately. They don’t understand most of the dialects spoken in Uganda, they haven’t eaten properly for a while, they hitchhiked – they are anxious and distressed,”. Namuyobo explained.
New arrivals, particularly women and young people, are welcomed into the safe space at the end of often long and difficult journeys.
While comprehensive data are unavailable, research and news reports have indicated women and young people face threats of gender-based violence and a lack of SRHI as they seek out better lives in the country.
To address these rights violations, RHU maintains 19 safe spaces across the country and the toll-free line (0800299003), where staff offer SRHI and work to identify instances of gender-based violence, offer case-management support, and refer survivors to corresponding public services. Teams also work with survivors to access health services, build safety plans, and monitor cases until resolution.
“RHU’s toll-free line and humanitarian response in Uganda is important to guarantee the health rights of marginalized and underserved people, especially young people, women, and girls,” said Tom Kulumba, who heads the RHU Gender and Youth department in Uganda.
In addition to sexual and reproductive health advice and gender-based violence support, each space accommodates breastfeeding mothers, and infant beds and provides free condoms and educational videos and games. Everyone is welcome, and the door is always open.
“Hundreds of vulnerable and underserved people have benefited from calling the RHU toll-free line,” Talent Emily, RHU toll-free line officer said. She contends that the callers are interested in family planning, infertility management, HIV, location of RU clinics, making appointments, and sexually transmitted infections (STI) management.
For some, this makes all the difference. “During an appointment, one woman mentioned her desire to use family planning,” Demeter Namuyobo recalled. “She put both hands on the table and said, ‘You are the first person so far who has looked at me, so I felt safe to open up – I think this is what sets us apart.”
As Ugandans face ongoing threats to their SRHI safety in some places – from a lack of essentials such as spaces, toll free lines, and medicine to political and socioeconomic crisis – RHU will continue its critical work of providing marginalized and vulnerable persons in their diversity a safe place to rest and recover.
The author Aldon Walukamba is a Media Advocacy and Documentation Coordinator at Reproductive Health Uganda

Why Family Planning Is Beneficial to Uganda’s development stride
Given the state of Uganda today, it is urgent that humanity and nature exist in balance. The burden, of course, is on the people to make this happen. In a country of 42.9 million people that could grow to 100 million by 2050, we are making this more difficult.
It doesn’t have to be that way. We know what must be done, but we must find the political and societal/cultural will to make it happen, in a manner that supports having a proper conversation about the best approaches. The solutions to attaining a healthy population count are grounded in the principles of rights and empowerment and are things the world should be doing anyway.
One of the first things to do is to invest in young people, who make up more than 75% of Uganda’s population and a population of 24 million women in health, particularly by providing deliberate and voluntary family planning services. This is often referred to as “low-hanging fruit,” because it is the right thing to do, relatively simple to provide, and something that most women and men desire. Everyone should have the right to plan if and when to have a family, and have the tools, resources, and access to do so, or not do so.
There are more than 23.19 million women in Uganda, including 10 million that are of reproductive age, but 17% want to delay or avoid pregnancy but are not using a modern contraceptive method. It is also true that 46 percent of Uganda’s estimated 36 births per thousand pregnancies in 2020 were unintended (PMA,2020).
The estimated current annual cost of providing modern contraceptive services in Uganda has gaps, including direct and indirect costs.
According to the National Family Planning (FP) Cost Implementation Plan (CIP) II (2021/22–2024/25), the overall funding need for FP commodities is the US $332.3 million. The government’s overall commitment to the reproductive health (RH) supplies budget over this time period, however, is the US $ 25 million. If this were to be expanded and improved to address all men and women’s needs for modern contraception in Uganda, a funding gap of US $ 307.3 million needs to be avoided.
Just to put that in perspective, the total per capita consumption of pure alcohol is 23.7 liters in Uganda. This approximately accounts for 480,000 shillings spent on alcohol by each Ugandan.
The government allocated a total of UGX 3.722 trillion for healthcare delivery in the financial year (FY) 2022/23. This has been largely geared towards the COVID-19 vaccination.
The good news is that with the celebration of 13 years of the Advance Family Planning initiative (AFP) in Uganda, the citizens know what to do, how to do it, and why to do it concerning family planning access. Let’s look at just two examples of why investing in family planning can make a huge difference in people’s lives in Uganda.
Most of the districts in Uganda are experiencing the highest rates of population growth in the world. In fact, Uganda’s population is expected to double, from 42.9 million today to 100 million by 2050. (UBOS, 2020)
One of the country’s fastest-growing populations in Wakiso. Its current population of 2.9 million is projected to reach 5.1 million by 2050, and it is one of Uganda’s youngest and most urbanized districts, with over 88 percent of the population under the age of 30. The district also has a number of street children and destitute.
One in four girls between the ages of 15 and 19 in Uganda has given birth or is carrying her first child, according to the United Nations Population Fund (UNFPA) country’s 2020 report. Reducing teen pregnancies will result in greater education and economic opportunities for young people. Meeting the reproductive rights and needs of youth through education, outreach, and access to services is imperative. Local organizations such as Reproductive Health Uganda and partners are working with youth to raise awareness and access to contraceptives and family planning services.
Unplanned teenage pregnancies account for 25% of all pregnancies in Uganda (PMA, 2020). The district of Iganga worked to change this situation through the Iganga Family Planning Initiative, which provided training, support, and low-or no-cost long-acting reversible contraceptives (LARCs) to low-income women, especially teens through the AFP and other interventions.
The Iganga district made more progress than any other district in using family planning to reduce unplanned pregnancies (UBOS, UNFPA, 2020). The district department of Health reported that teen pregnancies were nearly cut in half and that, ” the AFP initiative and other interventions empowered thousands of Iganga women to choose when and whether to start a family” Iganga’s experience is a model for other districts. They can now educate, treat and do other development activities with fewer, but manageable family sizes. If replicated, with fewer resources required to manage families, the surplus can go to agriculture, and business and help achieve Uganda’s national development plan III and vision 2040 indicators.
As we celebrate this year’s World Contraceptive Day on September 26, 2022, let’s focus on family planning as a development issue; make it visible; budget for it; and make policies that allow for its access in Uganda. It is good for the child, mother, father, and family.
The author of this opinion story Aldon Walukamba is a Media Advocacy and Documentation Coordinator at RHU
Operational Research (OR) on the implementation of meaningful inclusive youth participation (MIYP) in RHRN2 programme in Uganda, July 2022
Young people have a fundamental human right to participate in matters that affect their lives. Through active participation, young people are empowered to play a vital role in their own development as well as in that of their communities, helping them to learn vital life-skills, develop knowledge on human rights and promote civic space.
It is known that MIYP can help young people to become active agents and leaders in their communities, taking primary responsibility for making decisions on matters that affect them. MIYP is considered to be a crucial component in many youth SRHR programs. It has positive effects on empowerment and civic engagement of young people; on adult staff and organization’s capacity to institutionalize meaningful involvement of young people, and provide youth-sensitive SRHR interventions and achieve program objectives.
RHRN2 coalition partners would like to assess the implementation of MIYP in their activities for year 2022. Findings from this study will assist coalition partners to review planned activities and find ways of giving space to adolescents and youth to actively and meaningfully participate in the implementation of activities, especially those concerning promotion of SRHR information to young people in general. In addition, the study is expected to generate recommendations that promote participation of youth at the decision-making levels.
If this interests you, Please follow the following procedures to express interest;
- Download full TOR Here
- The OR should be completed by 31st Aug 2022. The total number of days for the OR are estimated to be 33 working days starting from 18th July.
- Interested persons should submit their technical and financial proposals to RHU Director of Programmes (DOP) at pibembe@rhu.or.ug and cc to Lawrence Muhangi (RHU M&E Manager) at lmuhangi@rhu.or.ug or hand deliver in person to RHU head office, plot 2, Katego Road, Kamwokya by close of business on Friday, 8th July, 2022 before 5:00pm.RHU will only contact eligible persons with whom further discussion is sought.

CONSULTANT TO CONDUCT THE REPRODUCTIVE HEALTH UGANDA (RHU) REORGANISATION, JOB EVALUATION AND GRADING, SALARY REVIEW AND PAY STRUCTURE
Reproductive Health Uganda (RHU) is a Member Association of the International Planned Parenthood Federation (IPPF), and its core mandate is to champion, provide and enable universal access to Sexual and Reproductive Health and Rights (SRHR) information and services to vulnerable and underserved communities, especially young people.
The Association has over 150 members of staff and over 4000 volunteers working with and for communities and individuals. RHU is also
committed to Universal Health Coverage (UHC) by contributing to the achievement of equitable access to life-saving, quality sexual and reproductive health care for all, including to the most marginalized and hard-to-reach population groups.
We are looking for a consultant/ firm to recommend a new or improved structure with roles that align well with the
organizational strategy, as well as conduct a Job Evaluation and Job Grading exercise, and Salaries and benefits review.
Application Process
Interested persons/consultancy firms must submit technical and financial proposals by Friday 24th June 2022 by 5:00pm to:
Office of the Executive Director, Reproductive Health Uganda Plot 2 Katego road, Off Kiira road, P.O Box 10746 Kampala
Tel: +256312207100/041 540658 Or Email: rhu@rhu.or.ug
RHU will contact persons with whom further discussion is sought. Please note that we may be unable to respond to applicants who have not been selected for interview.
RHU AND PARTNERS HOST THE UK ALL PARTY PARLIAMENTARY GROUP
RHU AND PARTNERS HOST A STUDY TOUR FOR THE UK ALL PARTY PARLIAMENTARY GROUP ON POPULATION, DEVELOPMENT & REPRODUCTIVE HEALTH
By Fortunate Kagumaho

A snap shot of the visit: LR; Jackson Chekweko attending to the head of the delegation. In the middle, Baroness at an RHU outreach. Hon Mp Luwero speaking to the Boda Boda men at the outreach
Earlier this month, Reproductive Health Uganda (RHU) and partners (Mariestopes and UNFPA) hosted the UK all party parliamentary group for a study tour. The team had an opportunity to visit the Uganda parliament, Ministry of Health and also some of our implementation sites
The visiting team was represented by Baroness Sugg. Baroness, a UK Parliamentarian, House of Lords and leader of the UK Parliamentarians delegation, said both Uganda and the UK need to support issues of women and girls, for the growth and development of both countries.
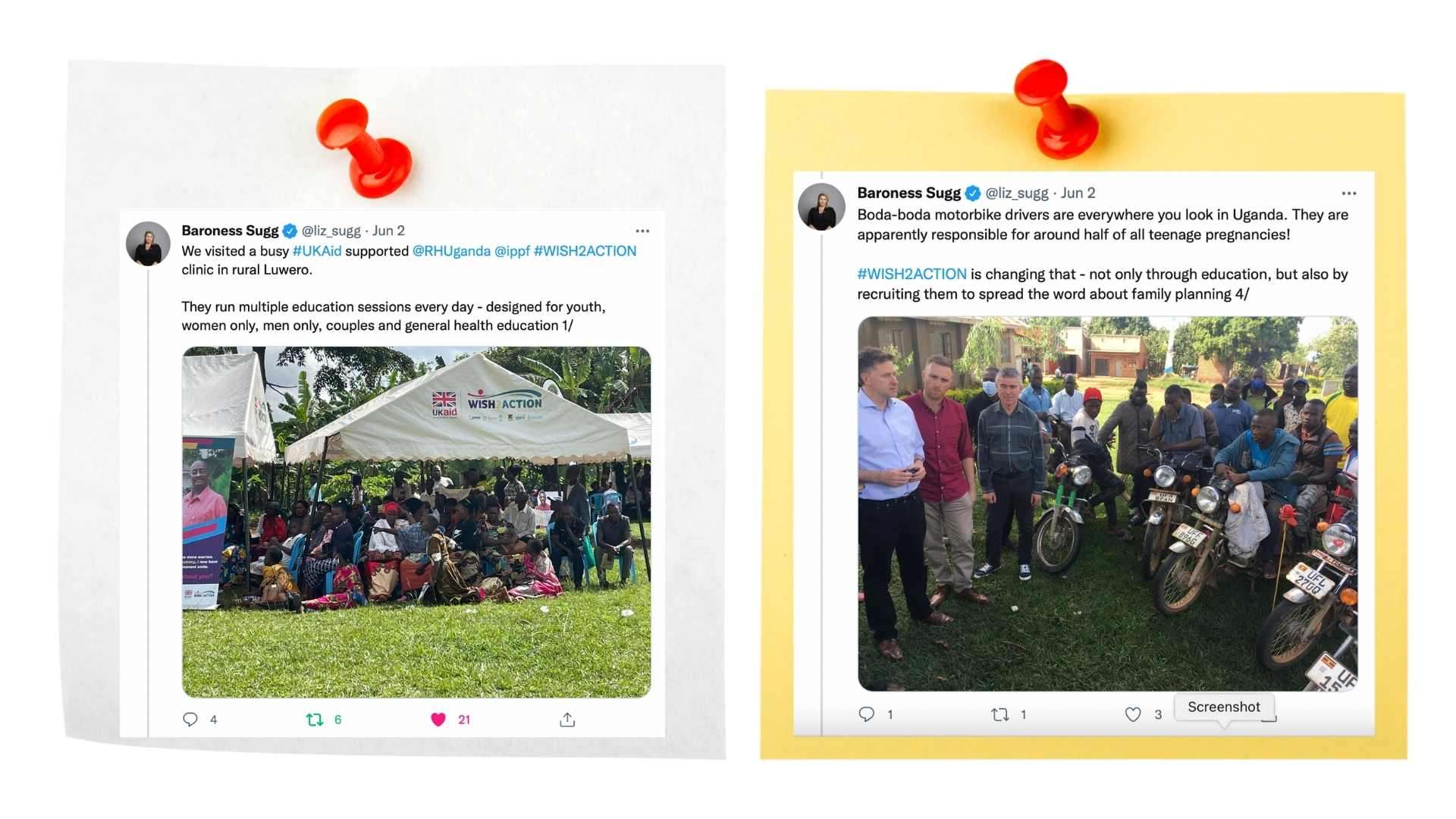
Baroness shared a tweet about her visit to the RHU outreach site
“We visited a busy UKAid supported RHU-WISH2ACTION clinic in rural Luwero. They run multiple education sessions every day – designed for youth, women only, men only, couples and general health education” Reported Baroness on her verified twitter handle.
She noted that the UK had developed an international development strategy, which among other highlights commitment made on programs on global health.
“We need to support their (women and girls) empowerment, prevent violence against women and girls and also help to educate girls. Our foreign secretary has made a commitment for more funding towards women and girls especially on issues of child marriages and female genital mutilation,” Baroness said.
Dr. Charles Ayume, the chairperson Parliamentary committee on health, told the meeting that there is need to invest in quality and healthy population for the development and growth of respective economies.
In response about the impact of COVID19 on the projects and how RHU handled, Dr Annet Nagudi (Project Director –WISH2ACTION) said,
“We experienced reduction in the number of clients at static service delivery points at the beginning of the lockdown. Team Resilience and positivity kept the project team going.” Said Dr Nagudi. “Travel clearances thanks to great collaboration with Ministry of Health -Uganda and the Districts, made our work even easier.” She added

“Our RHU team integrated COVID I9 in SBCC messaging and Budget adaptation thanks to donor flexibility which facilitated smooth continuity. We also RHU set up COVID 19 response team that guided continuity of services. We adopted National SOPs and disseminated these to all service delivery points. Community Outreach services and training of VHTs to deliver DMPA-SC facilitated continued access to Services.” Dr Nagudi said
Women’s Integrated Sexual Health Lot 2 Project (WISH2ACTION) is IPPFs flagship project aiming to transform the lives of millions of women and girls. Funded by The Foreign, Commonwealth & Development Office (FCDO), WISH2ACTION seeks to provide integrated and holistic reproductive healthcare to 2.2M additional users of contraception across 15 countries in Africa and South Asia from 2018 to 2022.
In Uganda, the project is implemented through its 6 consortium partners (Reproductive Health Uganda IPPF’s Member Association in Uganda, Marie Stopes International Uganda, International Rescue Committee, Development Media International, Humanity and Inclusion and Options working in 77 districts of Uganda aims to increase access to family planning services of the most marginalized including young people, people living in poverty and people with disabilities.
In collaboration with the Reproductive Health Directorate and other stakeholders such as community leaders, policy maker and CSOs the programme works towards enhancing a supportive legal, financial and policy framework for sustainable family planning and a conducive environment for SRHR for all women and girls so that they face fewer risks during pregnancy and childbirth.
Fortunate Kagumaho is the Communications Coordinator at Reproductive Health Uganda

CONSULTANCY NEEDED FOR EVALUATION OF AFP PROJECT IN UGANDA
Reproductive Health Uganda (RHU) and Partners in Population and Development (PPDAro) are looking for a consultant to conduct a summative evaluation for the Advance Family Planning project (AFP)
Overview of the Advance Family Planning Initiative in Uganda
Advance Family Planning (AFP) is an advocacy initiative of the Bill and Melinda Gates Institute for Population and Reproductive Health and the Johns Hopkins School of Public Health implemented in ten countries. The initiative was launched in Uganda in November 2009 with the aim of improving the funding and policy environment and galvanizing political commitment needed to ensure access to a full choice of family planning services and information. This is attained through collective efforts working with likeminded partners to build consensus, mostly targeting decision makers using a unique AFP SMART Advocacy approach.
The advocacy approach hinges on seven principles: locally-driven, focused, evidence-based, collaborative, influence, accountability and sustainability.
AFP works in collaboration with governments, donors, implementing partners, religious, media, and cultural institutions, as well as other state and non-state actors, to ensure that the country’s FP2030 commitments are met, as well as to track progress and understand advocacy priorities.
In Uganda, the AFP initiative is implemented by Reproductive Health Uganda (RHU) and Partners in Population and Development, Africa Region Office (PPDARO), working at both national and at Sub National level- over the years, engaging subnational decision
makers of 32 districts
Objectives of the Assignment
December 2022, marks the end of AFP implementation. Therefore, the main objective of the consultancy is to evaluate the performance, effectiveness, efficiency and impact of the AFP initiative in Uganda over the years.
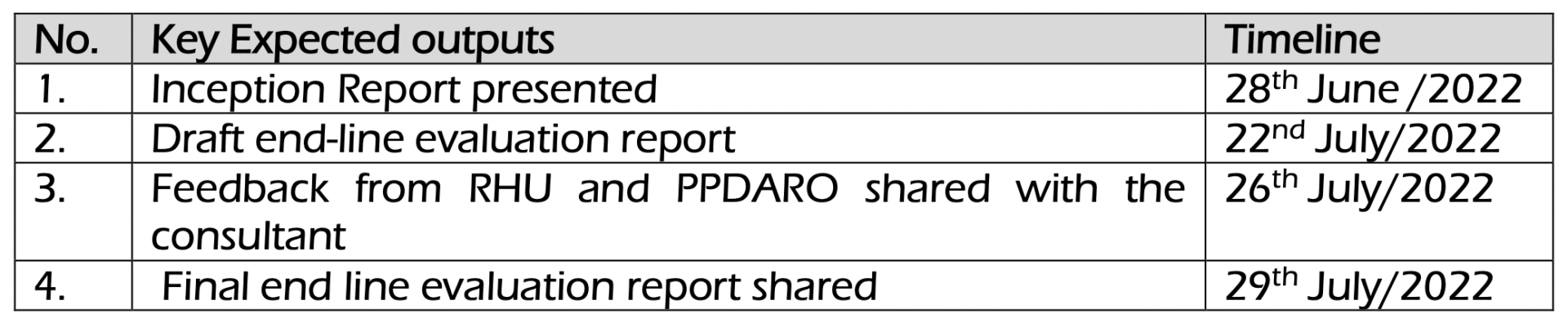
Deliverables/Expected Outputs and time lines
The consultant team is expected to produce the following;
TOR for documenting AFP work (Down load PDF here)
Application process
Interested persons should submit technical and financial proposals to the Executive Director, Reproductive Health Uganda – rhu@rhu.or.ug and copy dkansiime@rhu.or.ug , ekiggundu@rhu.or.ug , aro@ppdsec.org by Friday, 10th, June 2022 before 5:00pm
Qualifying candidates will be contacted by Friday 17th June, 2022.

Menstrual health needs surge among vulnerable people in Uganda
Uganda – The 2021 outbreak of violence in the Equatorial region of South Sudan has displaced inside South Sudan, nearly two million people while outside the country there are now over two million South Sudanese refugees, mainly in Ethiopia, Sudan, and Uganda. Many have fears of imminent attack or struggle with food insecurity, sexual reproductive health issues, trauma, and menstrual health among young girls and women. People were forced by over 35,000 to flee to Uganda, roughly 75 percent of refugees from South Sudan are women and children.
Women and girls displaced by conflict face extraordinary hardships in most refugee camps and urban areas of Uganda. Many endure grave risks, including gender-based violence, which can escalate in humanitarian settings. Most are thrust into poverty – cut off from education and life-saving health services, including menstrual health.
Displacement exacts another huge toll on women and girls. In the refugee camps and Uganda’s urban areas, their most intimate and taboo health needs are often overlooked, to devastating effect.
“I had my first period here at the settlement,” said Joyce Tabaria, 12, whose family now lives in the Ayillo II settlement, home to over 39,000 refugees. “I had no idea what was happening. For me, that day was sad and shameful.”
Stigmas surrounding menstruation have existed across cultures in Uganda, also affecting indigenous people and history has it that most people in the community neglect or don’t care about issues of menstrual hygiene. And it’s not uncommon for women and girls to internalize these destructive myths.
A report published by International Rescue Committee (IRC) earlier this year details the extent to which lack of menstrual care, period shame, and misinformation reinforce gender discrimination, rendering women and girls vulnerable to poverty, violence, and harmful practices.
The IRC report reads, “Out of the 79% women and girls that indicate experiencing menstrual pain, only 28% have access to pain killers. While right and adequate menstrual health hygiene (MHH) information are limited. For school girls, a major source of information is schools (61%), peers (45%), workmates (37%), and CSOs/NGOs (27%)”.
In Uganda, the idea that menstruating women and girls are unclean contributes to their exclusion not only from family life but also from education and employment.
Dr. Peter Ibembe, Reproductive Health Uganda (RHU) Director of Programs says that in some places, isolation and expulsion from the home can be dangerous, exposing women and girls to extreme weather and sexual violence.
“In others, the onset of menstruation is associated with child marriage, which heightens the risk of adolescent pregnancy and life-threatening complications before, during, and after childbirth” says Dr Ibembe.
According to some vulnerable refugees and displaced people in Uganda, displacement magnifies these conditions.
“When I’m menstruating, I usually use strips of absorbent cloth, but in the settlement, it is difficult to get this cloth,” Hellen Aleyo in Kasese told RHU.
The unmet needs for sexual and reproductive health services intensify for women and girls in exile. Refugees need to receive adequate care and access to dignity kits in the settlements.
Harmful conditions in evacuation sites can wreak havoc on women’s sexual and reproductive health, while lack of access to hygiene supplies limits their mobility and heightens their vulnerability to sexual violence. Girls who do not have the ability to manage their menstrual health are also at greater risk of missing school or dropping out entirely.
Hellen Furaha, is the recipient of one of the sexual reproductive health and rights (SRHR), menstrual health training, and dignity kits distributed to women and girls in the Muhookya internally displaced people’s settlement in the Kasese district. The kits contain essential hygiene items such as sanitary pads, underclothes, soap, toothbrushes, and toothpaste.
As we celebrate menstrual health month 2022, it is important to note that RHU works with partners SRHR Alliance with support from Rutgers to deliver dignity kits to women and girls around Uganda in schools and in women’s and girls’ safe spaces. These safe spaces provide more than sexual and reproductive health services.
Aldon Walukamba G, the author, is the RHU Media Advocacy and Documentation Coordinator.

Child bride and fistula survivor becomes an advocate for change
Uganda : Rachael Wotali, was just a teenager, married at 17, when she nearly died in childbirth.
It was the year 2015 in eastern Uganda’s Iganga District. Wotali, as a young bride, may have been biologically unprepared for motherhood.
Her labor was extended and blocked, which may have been fatal. Her access to emergency treatment was also critically hampered. She recalls her mother yelling with the health care provider over their extended wait for help.
Unfortunately, the baby died at birth, leaving Wotali with an obstetric fistula, a hole in the birth canal that rendered her incontinent and exposed to a variety of other medical issues, including infections.
“I never enjoyed being a woman in marriage since I had this condition,” she later recalled. “It was tough to live.”
Today, the 23rd April 2022 is International Day to Put an End to Obstetric Fistulas. Fistulas are one of the most dangerous and devastating delivery injuries, and they are virtually totally avoidable. Access to competent maternal health care, particularly Caesarean sections to treat obstructed labor, can save both women’s and their kids’ lives and health.
Although the prevalence of obstetric fistula in Uganda stands at two percent, a 2016 study by the Ministry of Health estimates 200,000 women are living with fistula, and 1,900 new cases occur each year.
Yet more than two million women in the developing world are estimated to be living with this condition. Its persistence is a sign that health and protection systems are failing women and girls.
Wotali lived with an obstetric fistula for six years. In that time, she had a son and a daughter. But, like many fistula survivors, she was isolated, enduring ridicule if she left home. She was unable to do community work, attend funerals or visit church, she told Reproductive Health Uganda (RHU), while receiving family planning.
Nothing appeared to work towards improving the situation. “Traditional herbalists tried everything, and we had been told to do lots of things but the condition was never healed,” she recalled. “When you are in that situation, you try almost everything.”
But one day, one year ago, her sister was chatting with community members at a nearby borehole. Someone mentioned that a woman in the district had received treatment for chronic urinary incontinence. It turned out a fistula repair camp was taking place at Iganga district hospital.
She rushed to tell her mother.
Over 25 women received treatment during the government – private partnership supported event, including Wotali.
“I am now dry. I have no problem,” Wotali said. “This is how a woman should be.”
Many of the women, like her, have endured the condition a long time. One Alowo, lived with fistula for 28 years in Mayuge district but was also treated.
We all need to take action against obstetric fistula. It is estimated that two per cent of women in the country have experienced an obstetric fistula, according to a 2016 survey.
Since her treatment, Wotali has become an advocate for fistula survivors, helping multiple women receive repairs.
She says she still thinks back to the fateful day that she learned there was hope and help for women with obstetric fistula.
“That morning when my sister went to draw water saved my life,” she said.
Aldon Walukamba G, the author, is the RHU Media Advocacy and Documentation Coordinator.

Girls fleeing from FGM in Uganda are directed to Safety
Uganda, Kampala – “With no safe houses- schools, girls will be genitally mutilated,” said 21- year old Ruth Chelangat a community mobiliser, who mobilizes girls against female genital mutilation (FGM) in Kwosir sub county in Kween district of Uganda’s largely rural Sebei region.
“You can’t receive protection in the neighborhood during the cutting season,” she stated.
In areas of Uganda where FGM is performed, the “cutting season” usually coincides with school holidays, as it is this year. FGM, which includes damaging or modifying the female genitalia for non-medical reasons, can have a variety of severe health repercussions for girls who are exposed to it, including pain, infections, hemorrhaging, and death.
But when Betty Cheboi, was 22 years old, she implored her parents not to have her cut. They didn’t listen, and she had no safe place to run to. She nearly bled to death from her wounds.
Afterwards, she made her close relatives promise not to cut her younger sisters. For Cheboi, it was the beginning of a lifetime of activism to end FGM.
After receiving training from the Right Here, Right Now II (RHRN II) and the United Nations Population Fund (UNFPA), several youth teams in the Karamoja and Sebei regions are spreading the word that girls can find refuge at the safe houses operated in Amudat and Kween districts through, school programs, young people’s safe spaces at health centers, and community outreach.
“this is part of our effort to change negative values, norms and rituals abusing the enjoyment of sexual reproductive health and rights, in addition to young people’s gender justice,” Cheboi said.
However, according to Joseph Cheptegei, Kwosir sub-county Community Development Officer, when a cry for aid comes in, whether from a girl at risk or a concerned community member, identifying the girl can be difficult. This is due to the geography in the Sebei area, extensive unmapped land in Karamoja, and a lack of connectivity, with settlements of up to 5,000 people without plots and never appearing on Google maps.
“We are coming together to widen our network to unite people against FGM from across the Karamoja and Sebei regions,” said Cheptegei.
RHRN II, UNFPA through Reproductive Health Uganda (RHU), has organized the volunteer network’s efforts to teach young people so that activists on the ground can better protect girls since 2016.
Samuel Musani, RHRN II officer in Sebei region says that trained volunteer mobilisers, peer educators and young advocates comb through villages of rural Sebei and Karamoja regions, tracing for girls at risk or threat of FGM. They are then referred to safe houses and schools constructed by Action Aid – Uganda, Ministry of Gender, Labor and Social Development (MGLSD).
RHU works with government and other private partners like Reach a Hand Uganda (RAHU), Action Aid and Kapchorwa Civil Society Association.
During the 2021, over 2,000 volunteers in over 60 sub counties were trained under the RHRN II and UNFPA programmes by RHU and its partners.
As more and more communities abandon FGM, programming needs to zero in on remaining hotspots, noted Jackson Chekweko, RHU Executive Director.
When the cutting season is complete, most girls return home after two months. Volunteers, community social welfare personnel, and specially trained police engage with families and communities to alter attitudes, a step toward changing the societal norms that maintain FGM.
“We talk to parents,” said Chebot. “We show them that FGM has effects and is illegal in Uganda.”
Girls can return home if their parents promise to honor their requests not to be cut off and to help them in continuing their education. Every three months, the program does a check-in with the girls.
Girls whose families refuse to reconcile are housed in safe houses, where they get therapy and continue their education. Chebot, on the other hand, does not give up attempting to persuade their families to alter their beliefs.
“We are not stopping,” she said. “We keep visiting those families, talking to them so we can have reconciliation.”
While officiating the anti FGM day celebrations in Kapchorwa, on 20th April 2022, Uganda’s State Minister for Gender and Culture Peace Regis Mutuuzo, pledged that the 2010 anti FGM law will be revised to curb the new trends, that aid FGM to be done in countries neighboring Uganda.
Aldon Walukamba G, the author, is the RHU Media Advocacy and Documentation Coordinator.

Ugandan Youths Serve as Gender Justice and SRHR Advocates
There is hope that gender justice, sexual reproductive health, and rights (SRHR) initiatives in Uganda will enjoy wider acceptance by having young people act as “envoys.”
The youths in the Rwenzori region of Uganda are taking the lead in this by forming groups and preaching the SRHR and gender justice gospel, rehabilitating school dropouts and drug and alcohol abusers, mostly aged between 10 and 24 years.
Mary Karungi, 22, of Kaguma village, received training in sensitizing and mobilizing young people about their sexuality, reproductive health rights, and how to avoid emergency situations caused by unplanned sex encounters.
This was after several young people in her village, some of whom were under the age of 18, became pregnant, married, and dropped out of school.
She believes that the time has come for young people to take the lead in educating others about the dangers of unplanned sex, pregnancy, and marriage.
“We are doing some work in the villages, we talk to young people about body changes and how to act when they manifest, use family planning for those who are sexually active, and also demystify the negative norms and values that encourage teenage pregnancy and early marriages,” Karungi said.
In the last three months, Karungi has reached out to 86 young people in her village.
Rachael Mbonabana, Kicwamba Health Youth Development Group Chairperson in Kabarole district, says more than 800 young people have been approached by their group of 12 members. They go to schools, churches, mosques, playgrounds, and other communal gatherings with a message about positive living by empowering youths to claim their SRHR and gender justice. They also offer free condom distribution, sexuality education, and other messages promoting positive gender equality norms and values.
But Hassan Sebugwaawo, a Right Here Right Now-2 coalition (RHRN-2) project officer for Reproductive Health Uganda (RHU) in the Rwenzori region, says 144 young people in 12 groups of 12 young people each were empowered to saturate the gospel of gender justice, equality, and SRHR among young people.
Youth of Destiny is another young people’s group in Fort Portal City, Kabarole district, making strides towards emancipating young people about their SRHR and gender equality positive norms and values.
Brain Murungi, a spokesperson for Youth of Destiny, said they have rehabilitated a formerly 12-year-old girl who had been married off during the COVID-19 lockdown and a former school dropout, a boy. The two are now studying at Mukungwe primary school. The girl enrolled in family planning because she is sexually active.
Claire Kagaaju, a Youth Advisory Committee (YAC) Chairperson embraces SRHR and Gender justice training for young people that is accelerating the spread of SRHR and gender equality messages in a more diversified manner among young people in Tooro region.
Dr. Peter Ibembe, (RHU), Director of Programs, grins with optimism that when more skills are continually imparted to youths regarding gender justice and SRHR, several young people will avoid early sex, pregnancy, and marriage and live a better and more meaningful life. The youths are trained in positioning themselves in various working groups in the public and private sector to push for access to SRHR, gender justice, and family planning methods, including the use of contraceptives.
Jackson Chekweko, RHU Executive Director, believes young people should continue to receive training from SRHR and gender justice professionals on communication, resource mobilization, and advocacy techniques. The youth envoys will then use these skills to lead discussions among local, religious, and cultural leaders to change bad norms and values affecting gender equality, SRHR, and justice.
“Emphasis to the youths is geared towards firming up civil society, so we work in coalition, to have the participation of not only youths, but also religious leaders and community leaders to push acceptance that takes into account the social, cultural, and religious contexts and work with an understanding of that to develop programs and activities even in rural areas of the country,” said Jackson Chekweko.
The RHRN-2 coalition comprises seven members including Reproductive Health Uganda (RHU), SRHR Alliance, Sexual Minorities Uganda (SMUG), Hope Mbale, CEHURD, Reach a Hand Uganda (RAHU), and UNYPA.
Aldon Walukamba G, the author, is the RHU Media Advocacy and Documentation Coordinator.