Featured Slider
Category:
Getting Cultural leaders on Board
At Reproductive Health Uganda, we strongly believe that especially local leaders are pivotal and key in promoting family planning in their communities. We have been engaging the different leaders in the communities around Uganda, see article from one of the major ones from Lango culture.
See attached excerpt from the biggest news paper in Uganda

No schools, no blood: How Covid-19 closure has worsened shortage
No schools, no blood: How Covid-19 closure has worsened shortage
Written by BY GILLIAN NANTUME – September 7th, Daily Monitor , Uganda
Reproductive Health Uganda through the SET SRHR project is advocating for increased funding to the National blood bank. This is through a campaign dabbed Saving lives through greater investment in safe blood transfusion services. Join the conversation on social media using #SupportTheUGBloodBank #SaveLives #WeAreRHU
Blood transfusions are a strong pillar in modern medicine and they have saved the lives of countless people. Women with pregnancy related complications, need donated blood more than all other groups, except children below the age of five. Dr Elizabeth Nabiwemba, the project director of SET-SRHR, says blood loss mainly affects women in childbirth because their blood levels are already low due to the pregnancy.
Who is at risk
“Haemorrhage is the number one killer of pregnant women. When there is no blood in a hospital the risk of a woman dying in labour is very high. She does not have to lose much blood to die.”
Sarah Mutegombwa, the programme manager for blood donor recruitment at Uganda Red Cross Society (URCS) says most of the donated blood goes to children below five years.
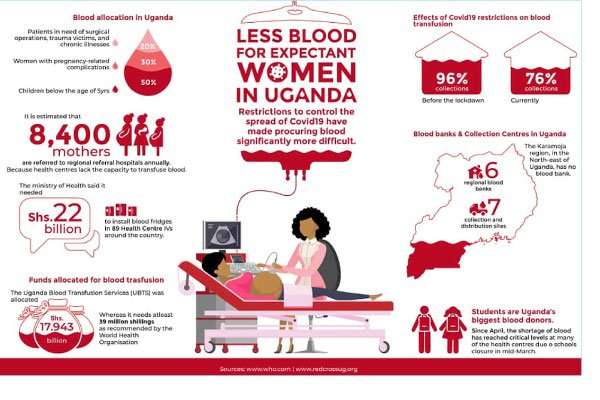
“These children take at least 50 percent of the blood because they become anaemic when they suffer from severe malaria and malnutrition. Women with pregnancy-related complications take up 30 percent of the demand, while the remaining 20 percent is shared by those in need of surgical operations, trauma victims, and those who suffer from chronic illnesses, such as cancer and sickle cell disease.”
Mutegombwa adds that one unit of blood can serve three children, because they use only one or two components of the blood, such as red blood cells, platelets, or the plasma. An adult, though, can consume as many whole units of blood as the need arises. In contrast, in high-income countries about 76 percent of the donated blood is received by patient groups over the age of 65.
Before the COVID-19 pandemic dominated the focus of health policymakers, the Ministry of Health (MoH) had, in its 2020/21 budget, said it would target equipping Level IV Health Centres to provide blood transfusion services in order to improve reproductive, maternal, neonatal, child and adolescent health services.
According to the Health Ministerial Policy Statement for the Financial Year 2020/2021, it is estimated that 8,400 mothers are referred to regional referral hospitals annually because Level IV Health Centres lack the capacity to perform obstetric care as they cannot transfuse blood. The ministry said it needed Shs2.2 Bn to install blood fridges in 89 Level IV Health Centres around the country.
Chronic blood shortages worsened
There are seven blood collection and distribution sites located in the districts of Lira, Nebbi, Jinja, Masaka, Kampala, and Hoima. The collections sites are not fully-fledged blood banks because they do not have testing facilities. Restrictions to control the spread of the coronavirus have made procuring blood, even from these few points, significantly more difficult.
While anyone between 17- 60 years can donate blood as long as they are in good health, students are Uganda’s biggest blood donors.
“During the school term, we run continuous blood donation mobilisations to replenish what is in the blood banks, until the students get holidays. As a country, we have been getting 70 percent of our total blood donations from schools. The remaining 30 per cent is collected from the community. Some areas organise and then, call us, with the intention of donating blood,” Mutegombwa says.
She adds that in schools, more boys donate blood than girls. “For girls, the barriers to donating are many. For instance, she cannot donate blood if she has recently completed her period because she has lost blood. Also, in the communities, there are restrictions on a pregnant woman and breastfeeding mother donating blood.
However, when in terms of the HIV prevalence rate, we target low risk donors, where the rate of infection is too small. Before we go to a community, we screen its prevalence levels and also give community members information so they can self-exclude themselves.”
Blood has a shelf life of 35 days. Schools were closed in mid-March. Since April, the shortage of blood has reached critical levels at many of the health centres. This shortage gives unscrupulous health workers an opportunity to raise the price of the few units of blood available.
“During the holidays, we would shift the blood donation mobilisation drives to the communities. But, the pandemic broke out during the school term, so we had to quickly switch to the communities. Unfortunately, we ended up with a [total] lockdown,” Mutegombwa says.
Who has been donating?
With the broader lockdown came bans on public gatherings and public and private transport. URCS switched to soliciting for blood from individual registered donors.
Uganda has between 80,000 and 90,000 registered blood donors, most of who donate twice a year. Mutegombwa says: “We would call a donor, pick them from home and drive them to our offices. After the donation, we took them back home.
Sometimes, we spent one hour on transporting a donor. On average, we would pick up between 20 to 30 donors per day. Each of these can only donate one unit of blood every three months if they are male or every four months if they are female.”
Cost of blood supply
The government meets the costs of blood donation. But sometimes, especially during the lockdown, groups such as the Indian Association, offered to transport blood donors.
Although both public and private transport are operational, blood donations are still low due to the restrictions on public gatherings in communities, and also, due to the fact that schools are still closed. Mutegombwa says prior to Covid19, their outreach teams would hold at least 30-40 minute-long awareness campaigns in a month, targeting at least 100 people but now it is difficult to organise more than 20 people in one place.
The bleeding processes (drawing blood from a donor) also takes much longer. Previously, one nurse could tend to two donors at the same time. Now, due to the physical distancing and other Covid19 related regulations, a nurse will spend about 15 minutes bleeding one person.
Dr Mathias Lugolobi is District Health Officer in Wakiso. He says, “We have four government and eight church-based facilities that can perform blood transfusions. Ideally, each facility needs 30 blood units per month.”
However, they never get that many units and Lugoloobi adds that during the lockdown the blood supply dwindled to the bare minimum. When there are shortages of blood, smaller health centres outside the main urban areas are de-prioritised.
Dr Francis Kakooza, the Kayunga District Health Officer is also in charge of its general hospital. He says his hospital gets only about 15 to 20 units a week yet, ideally, they need 30 to 40 units. In times of shortages they do not get any blood from Nakasero blood bank.
“At times, we only get 10 units. So, we transfer patients who need blood to Jinja or Kampala districts. However, at the peak of the lockdown, we only made referrals to Kampala because in most cases, Jinja also suffered blood shortages. Right now, we are renovating the hospital and soon we will have an emergency trauma unit. This means we will need more blood,” he says.
The WHO standard
The Uganda Blood Transfusion Services (UBTS), the institution mandated to collect, test, store and distribute blood was allocated Shs17.824 billion (USD 4.8 million) in the 2020/2021 Financial Year. Of this amount, Shs 4.9 billion will go to wages and salaries, Shs 4.758 billion on travel and transport, Shs 2.675billion on general expenses, Shs 1.479billion on maintenance, and only Shs 476 million on supplies and services.
According to the World Health Organisation’s Global Database on Blood Safety, a country should be able to collect blood equivalent to one percent of its population. Uganda has an estimated population of 45,903,545 people.
This means the country needs to collect 459,035 units of blood annually. According to URCS, it costs USD85 (Shs 331,500) to collect one unit of blood. This means UBTS needs USD 39 million (Shs152.1 billion) if it were to meet the WHO recommendations. Mutegombwa says that the country is not set to meet the WHO target at the moment.
“Instead of the 459,035 units of blood, our target is 300,000 units a year,” she says.
That target, which translates into 25,000 units a month, is also often missed. By the end of last year, only 288,000 units had been collected,” she says.
Coronavirus restrictions made a bad situation worse. “Before the lockdown, as a country, we were at 96 percent collections. Currently, we are at 76 per cent. In April, only 14,768 units were collected, 23,032 units were collected in May and 19,050 units in June,” Mutegombwa adds.
Blood donation drive
The blood shortage has motivated medical doctors to fundraise for blood. Dr Joseph Gavin Nyanzi, the in-charge of Cherish Health Centre, a private-not- for-profit facility in Garuga, Wakiso district, has partnered with the Rotary Blood Bank at Mengo Hospital in a donation drive. Dr Nyanzi is also the public relations officer of the Uganda Medical Association.
“Over time, I have realised the need of blood as a medical product. So, on July 31, to commemorate my mother’s 70th birthday, I started a drive. My target is to collect 140 units of blood by September 3, when the drive will end. As of today (August 16) we have collected 20 units. Everyone is welcome to donate blood from Monday to Friday at the Rotary Blood Bank,” he says.
This is the second time Dr Nyanzi is carrying out a . In January last year, his drive had a target of 105 units but he managed to collect 16 units.
“There is only one factory of blood – you and I. If you donate blood, you also get the satisfaction of knowing your blood can make the different between life and death for someone,” he says.
Charting a way forward
On July 16, 2020, the UBTS appeared before Parliament’s health committee and requested for Shs20.5 billion to mitigate the blood shortage. Of this amount, Shs 10 billion wasww to offset a previous debt while the remaining Shs 10 billion was to help UBTS in the current crisis. The money has not yet been received.
However, there is a general feeling that UBTS is getting a lot of money but the problem is with prioritising how the money should be used. With prioritising blood collection, testing and distributing, the Ministry of Finance can be convinced when it comes to the supplementary budget. But the problem isn’t always financial. Mutegombwa says the majority of the registered donors are students.
“Adults fear donating blood because they do not want to know their HIV status. Some believe their blood supply will dwindle if they donate. Lack of information, discouraging cultural and religious beliefs about blood donation is also a hindrance. People see blood donation as taboo. They associate it with human sacrifice!” Mutegombwa says. Dr Nabiwemba says the general community should be mobilised.
“I know a woman who went to her church and talked to the congregants about the blood shortage. She asked them to bring other friends to donate blood in two weeks’ time and it was a successful donation. I think we can do this even in this era of social distancing. We can donate while observing the standard operating procedures.”
According to a Memorandum of Understanding signed between the Ministry of Health and URCS and UBTS, the two organisations are working with village health teams to register potential donors in rural areas.
To engage the public, the URSC has developed the Blood for Uganda App for both android and iOS which people can download and get to know the blood donation sites near them.
Mutegombwa says 114 donors have so far registered with the App. “When there is a need for blood from rare blood types, we activate the contacts in the App and they come to our offices to donate because most of them are walk-in donors.”
The app also creates a database of volunteers who can be reached in time of need and to achieve the No shortage of Blood goal. However, the App can only apply to people who use smartphones. Those who do not have them, have to rely on the honesty of medical workers.
#SupportTheUGBloodBank #SaveLives
Saving lives through greater investment in safe blood transfusion services
#SupportTheUGBloodBank #SaveLives #WeAreRHU
Join the conversation on social media,using #SupportTheUGBloodBank #SaveLives #WeAreRHU
Did you know: It is not enough to just donate blood? See why it is important to donate and get on board. Change starts with you, you never know when you will need the blood.
Background and context
The Government of Uganda has made significant strides in providing access to safe and sufficient blood to Ugandans who need it. Data from Uganda Blood Transfusion Services (UBTS) shows that the total units of blood collected annually has increased from 131,226 in 2007/2008 to 274,308 in 2018/19 Financial Year. Regional blood banks have been established in 7 locations; blood collection centres have also been set up in 9 other locations and the national blood bank at Nakasero has been revamped to provide better services. Government has gradually increased funding for blood, especially following the exit of PEPFAR in 2017 e.g. from Uganda Shillings 23.815 billion in FY 2016/17 to 46.94 billion in FY 2019/2020. The Ministry of Health Annual Report of 2017/2018 shows that 87 (48%) of the country’s 187 HCIVs were offering Comprehensive Emergency Obstetric Care (CEmOC) in 2018, having increased from 44.6% in 2016/17 FY and blood transfusion is a key requirement in the provision of CEmOC. Increased access to blood has contributed to a reduction in maternal mortality from 418 per 100,000 live births in 2006 to 368 in 2016; and a reduction in child mortality rates between 1995 and 2016 from 156 to 64 per 1,000 live births among others.
Cause for concern?
 Despite the aforementioned progress, significant challenges persist. Recent engagement between UBTS and selected Civil society organisations highlighted a number of teething challenges: such as inadequate funding i.e. if UBTS is to collect 495,030 Units of blood (as per WHO requirement of 1% of the Uganda population) at 80.8[1] USD a unit, it will need Uganda Shillings 156 billion in 2021[2]. This is 3 times more than the current funding of Uganda Shillings 46.94 billion (Exchange rate of MoF-3900 Ugx/1USD)[3]. There is inadequate infrastructure- e.g. inadequate storage facilities for blood and medical supplies in many of the Regional Blood Banks; inadequate transport and staffing to meet the desired collection and supply target among others;
Despite the aforementioned progress, significant challenges persist. Recent engagement between UBTS and selected Civil society organisations highlighted a number of teething challenges: such as inadequate funding i.e. if UBTS is to collect 495,030 Units of blood (as per WHO requirement of 1% of the Uganda population) at 80.8[1] USD a unit, it will need Uganda Shillings 156 billion in 2021[2]. This is 3 times more than the current funding of Uganda Shillings 46.94 billion (Exchange rate of MoF-3900 Ugx/1USD)[3]. There is inadequate infrastructure- e.g. inadequate storage facilities for blood and medical supplies in many of the Regional Blood Banks; inadequate transport and staffing to meet the desired collection and supply target among others;
The catch?
Indeed, Uganda will not attain the goal of universal health coverage without addressing the myriad of challenges associated with supply and distribution of blood at all levels of the health system. Data from UBTS shows that a total of 274,308 Units of blood was collected in 2018/19 representing approximately 60% of the country’s total blood requirement during the year. UBTS estimates that Uganda will require 495,030 Units of blood in 2021 and 510,030 in 2022 based on current population growth projection. Currently, 29% of the total blood collected is used for treating people with severe malaria; 17% is for treating pregnant women with anaemia and complications of child birth; 17% for treating people with sickle cell anaemia, 15% for treating cancer cases, 6% for accident cases and 16% for treating other cases (burns, surgical operations) (UBTS).
Ensuring affordable, accessible, acceptable and good quality health care for all Uganda’s will reduce the inequality gap but also ensure that key programmes like UBTS are efficient in tackling the persistent service delivery challenges in the health sector.
Our plan!
The national policy dialogue on availability and accessibility to safe blood for improved maternal health outcomes in Uganda is being organised against the backdrop of persistent media reports of blood shortage in some public health facilities which has led to avoidable maternal deaths at such facilities. This situation has been exacerbated by the COVID 19 pandemic which has brought severe restrictions on gatherings like schools and other community mobilisations which were the major platforms for blood donation drives. In the recent past, MoH has sought additional 20.5 billion shillings in supplementary budget allocation to fund blood collection during the COVID-19 lock down. While this is a welcome relief especially if it’s approved and the funds made available to the Ministry, it does not address the recurring problem of under funding of blood collection and maternal health services generally. There is need for significant and sustainable financing for UBTS and blood transfusion services beyond the firefighting approach through the supplementary allocations.
This dialogue will build on and reinforce the ongoing civil society campaigns led by CEHURD which calls for increased government funding for blood and blood transfusion services, especially following the exit of PEPFAR in 2017. The dialogue which will be held on mass media (TV, Print/online, and social media) is being organised by Reproductive Health Uganda (RHU) and Makerere University School of Public Health (MakSPH) under the SETSRHR project in collaboration with Centre for Human Rights and Development (CEHURD).
Objectives of the dialogue
Organized under the theme: Saving Lives through greater investment in safe blood transfusion services, the national policy dialogue seeks to mobilize support for and increase commitment towards the achievement of universal access to safe blood transfusion services and improve health outcomes in the country. To that end, the policy dialogue aims to achieve the following specific objectives:
- To highlight the persistent challenge of blood shortage and access to blood in our health system and how these are undermining national efforts to address maternal morbidity and mortality.
- To provide opportunity for policy makers, practitioners and beneficiaries to examine the underlying issues underpinning blood shortage and blood access in our health system and how these can be addressed in a sustainable manner;
- Advocate for adequate and sustainable financing for blood transfusion services and maternal health services generally;
- Strengthen partnerships between relevant government agencies (at national and sub-national levels), civil society organisations and private sector for effective and efficient delivery of blood transfusion services in the country.
The road map
-
- Special report: under the headline “no woman should die giving life”, the special report will be based on observations at selected health facilities and experiences of/interviews with health policy makers, service providers, opinion leaders and end users. It will highlight the issues related to availability and access to safe blood from the perspective of policy makers, service providers, blood donors and end users. The report will be aired on NBS Television and preceding the talkshows.
- Television talk Shows: a total of 3 talk shows will be conducted on NBSTV. It will build on the investigative stories. Each talk show will examine the issue of availability and access to safe blood from different perspectives.
- The first talk show will focus at the macro-level looking at the national requirements, current provisions, enabling policies, gaps and challenges in human resources, financing, partnerships, technical support and opportunities for improvements
- The second talk show will delve into the technical and operational challenges faced by frontline service providers in ensuring adequate, timely and quality blood transfusion services and the opportunities for addressing identified gaps
- The third and last talk show will look at the demand side constraints focusing on the experiences of end users and how these can be addressed. The talk shows will be simultaneously relayed on selected radio stations.
- Newspaper publications: newspaper articles will be based on data and information from field interviews (policy and decision makers, service providers and end users) and review of secondary data from published sources. The articles will be published in the 2 leading dailies-New vision and Daily Monitor. The newspaper articles will be published during the same week as the TV talk shows and will mirror the themes addressed by the TV talk shows. The newspaper articles will be written by leading journalists from New vision and Monitor publications.
- Promotional adverts: the adverts will run on NBS for a period of 1 month and will aim at promoting blood donation in the country and mobilising communities for this.
- Social media engagements: The 3 TV talk shows discussions and corresponding donation drive adverts will be highlighted on different social media platforms; Twitter: @nbstv; @SolomonSerwanjj; @RHUganda; @cehurduganda; @SETSRHRUg. Facebook: @rhuganda; @CehurdUG. This will give the public an opportunity to contribute to the discussions at hand and also be involved in the donation drives.
- Participants for the Talk Shows
- Talk show moderator: The talk shows will be moderated by Solomon Serwanja, a seasoned investigative journalist and news anchor with NBSTV. In 2019 Serwanjja was awarded the Komla Dumor Award, an annual award given by the BBC to celebrate African journalists. He is also very passionate and vocal about the issue of access to blood and issues around maternal and reproductive health. Solomon will also lead the TV investigative story coverage.
5.2 First Talk Show Panellists
- In the Studio: The Chair of the Parliamentary Committee on Health – Michael Bukenya, Permanent secretary MoH – Dr. Diana Atwine, and Executive Director, UBTS, Dr. Dorothy Kyeyune.
- Via Zoom: Executive Director RHU, Mr. Jackson Chekweko, and Executive Director CSBAG.
5.3 Second Talk show Panellists
- In the studio: Director Health Services, Ministry of Health, Charles Olaro, Relevant Technical Officer from UBTS – TBC, Director Arua regional Referral Hospital –Dr. Philbert Nyeko
- Via zoom: Executive Director CEHURD – Moses Mulumba, and Representative from Uganda Red Cross Society and Rep. from Mengo Hospital.
5.3 Third Talk Show Panellists;
- In the Studio: Director Obstetrics and Gynaecology Mulago Hospital – Professor Annet Nakimuli, representative of health Consumers, Representative of UBTS
- Via Zoom: someone with extensive relevant research, President of the Uganda Obstetrics and Gynaecology Association -TBC, Private sector
On social media, the conversation will use #SupportTheUGBloodBank #SaveLives #WeAreRHU

Tips for working from home successfully
Following the outbreak of the Novel Corona virus world wide, most of us have been forced to work from home. We have come up with a few tips to help you work efficiently and effectively from home. Click here to learn more RHU-ICT-COVID-19 WFH

Not ready to get pregnant yet? Here are a few things you could do
These are very unprecedented times. We are no longer dealing with the same challenges as we were before. Times where we knew how not to spread HIV/AIDS or at least contain it. We could easily treat or prevent Sexually Transmitted Infections and disease (STDs/STIs). And now? Chlamydia, Gonorrhoea, Syphilis and even THE HIV/AIDs itself are no match for the Novel Corona virus.
These are indeed very uncertain times, with governments all over the world taking drastic measures to lock down, restrict movements and yet with diminutive hope or certainty that things will go back to normal soon.
Take caution :
With most people working from home or on forced leave and movement restrictions, loneliness, boredom with the so much time is paramount. For those staying with their partners the idea of sex must be flaunting. I mean ‘things’ are freely available on full time basis right?
Please note: Even if you are under self or institutional quarantine, having unprotected sex will still expose you to STIs and STDs and unplanned pregnancies.
But since abstinence is a complicated subject even without the CORONA virus, how can one enjoy their things without fear of getting pregnant or contracting STDS or STIs?
How do i not get pregnant?
Using contraceptives allows people to attain their desired number of children and determine the spacing of pregnancies. They are also very helpful in times such as these where one wouldn’t want to get pregnant.
There are however two methods one can use to delay pregnancy; Traditional and modern methods these are broken down below;
Reproductive Health Uganda clinics remain open across the country You can call any of the clinics in charges for appointments and or questions
What are the Modern methods?
PS: We recommend using modern methods because of their accuracy. They can easily be relied on without fear. These methods are available at any of the Reproductive Health Clinics countrywide. Give us a call to make an appointment
| Method | Description | How it works | Effectiveness to prevent pregnancy | Comments | |
| Combined oral contraceptives (COCs) or “the pill” | Contains two hormones (estrogen and progestogen) | Prevents the release of eggs from the ovaries (ovulation) | >99% with correct and consistent use | Reduces risk of endometrial and ovarian cancer | |
| 92% as commonly used | |||||
| Progestogen-only pills (POPs) or “the minipill” | Contains only progestogen hormone, not estrogen | Thickens cervical mucous to block sperm and egg from meeting and prevents ovulation | 99% with correct and consistent use | Can be used while breastfeeding; must be taken at the same time each day | |
| 90–97% as commonly used | |||||
| Implants | Small, flexible rods or capsules placed under the skin of the upper arm; contains progestogen hormone only | Thickens cervical mucous to block sperm and egg from meeting and prevents ovulation | >99% | Health-care provider must insert and remove; can be used for 3–5 years depending on implant; irregular vaginal bleeding common but not harmful | |
| Progestogen only injectables | Injected into the muscle or under the skin every 2 or 3 months, depending on product | Thickens cervical mucous to block sperm and egg from meeting and prevents ovulation | >99% with correct and consistent use | Delayed return to fertility (about 1–4 months on the average) after use; irregular vaginal bleeding common, but not harmful | |
| 97% as commonly used | |||||
| Monthly injectables or combined injectable contraceptives (CIC) | Injected monthly into the muscle, contains estrogen and progestogen | Prevents the release of eggs from the ovaries (ovulation) | >99% with correct and consistent use | Irregular vaginal bleeding common, but not harmful | |
| 97% as commonly used | |||||
| Combined contraceptive patch and combined contraceptive vaginal ring (CVR) | Continuously releases 2 hormones – a progestin and an estrogen- directly through the skin (patch) or from the ring. | Prevents the release of eggs from the ovaries (ovulation) | The patch and the CVR are new and research on effectiveness is limited. Effectiveness studies report that it may be more effective than the COCs, both as commonly and consistent or correct use. | The Patch and the CVR provide a comparable safety and pharmacokinetic profile to COCs with similar hormone formulations. | |
| Intrauterine device (IUD): copper containing | Small flexible plastic device containing copper sleeves or wire that is inserted into the uterus | Copper component damages sperm and prevents it from meeting the egg | >99% | Longer and heavier periods during first months of use are common but not harmful; can also be used as emergency contraception | |
| Intrauterine device (IUD) levonorgestrel | A T-shaped plastic device inserted into the uterus that steadily releases small amounts of levonorgestrel each day | Thickens cervical mucous to block sperm and egg from meeting | >99% | Decreases amount of blood lost with menstruation over time; Reduces menstrual cramps and symptoms of endometriosis; amenorrhea (no menstrual bleeding) in a group of users | |
| Male condoms | Sheaths or coverings that fit over a man’s erect penis | Forms a barrier to prevent sperm and egg from meeting | 98% with correct and consistent use | Also protects against sexually transmitted infections, including HIV | |
| 85% as commonly used | |||||
| Female condoms | Sheaths, or linings, that fit loosely inside a woman’s vagina, made of thin, transparent, soft plastic film | Forms a barrier to prevent sperm and egg from meeting | 90% with correct and consistent use | Also protects against sexually transmitted infections, including HIV | |
| 79% as commonly used | |||||
| Male sterilization (vasectomy) | Permanent contraception to block or cut the vas deferens tubes that carry sperm from the testicles | Keeps sperm out of ejaculated semen | >99% after 3 months semen evaluation | 3 months delay in taking effect while stored sperm is still present; does not affect male sexual performance; voluntary and informed choice is essential | |
| 97–98% with no semen evaluation | |||||
| Female sterilization (tubal ligation) | Permanent contraception to block or cut the fallopian tubes | Eggs are blocked from meeting sperm | >99% | Voluntary and informed choice is essential | |
| Lactational amenorrhea method (LAM) | Temporary contraception for new mothers whose monthly bleeding has not returned; requires exclusive or full breastfeeding day and night of an infant less than 6 months old | Prevents the release of eggs from the ovaries (ovulation) | 99% with correct and consistent use | A temporary family planning method based on the natural effect of breastfeeding on fertility | |
| 98% as commonly used | |||||
| Emergency contraception pills (ulipristal acetate 30 mg or levonorgestrel 1.5 mg) | Pills taken to prevent pregnancy up to 5 days after unprotected sex | Delays ovulation | If all 100 women used progestin-only emergency contraception, one would likely become pregnant. | Does not disrupt an already existing pregnancy | |
| Standard Days Method or SDM | Women track their fertile periods (usually days 8 to 19 of each 26 to 32 day cycle) using cycle beads or other aids | Prevents pregnancy by avoiding unprotected vaginal sex during most fertile days. | 95% with consistent and correct use. | Can be used to identify fertile days by both women who want to become pregnant and women who want to avoid pregnancy. Correct, consistent use requires partner cooperation. | |
| 88% with common use (Arevalo et al 2002) | |||||
| Basal Body Temperature (BBT) Method | Woman takes her body temperature at the same time each morning before getting out of bed observing for an increase of 0.2 to 0.5 degrees C. | Prevents pregnancy by avoiding unprotected vaginal sex during fertile days | 99% effective with correct and consistent use. | If the BBT has risen and has stayed higher for 3 full days, ovulation has occurred and the fertile period has passed. Sex can resume on the 4th day until her next monthly bleeding. | |
| 75% with typical use of FABM (Trussell, 2009) | |||||
| Two Day Method | Women track their fertile periods by observing presence of cervical mucus (if any type color or consistency) | Prevents pregnancy by avoiding unprotected vaginal sex during most fertile days, | 96% with correct and consistent use. | Difficult to use if a woman has a vaginal infection or another condition that changes cervical mucus. Unprotected coitus may be resumed after 2 consecutive dry days (or without secretions) | |
| 86% with typical or common use. (Arevalo, 2004) | |||||
| Sympto-thermal Method | Women track their fertile periods by observing changes in the cervical mucus (clear texture) , body temperature (slight increase) and consistency of the cervix (softening). | Prevents pregnancy by avoiding unprotected vaginal sex during most fertile | 98% with correct and consistent use. | May have to be used with caution after an abortion, around menarche or menopause, and in conditions which may increase body temperature. | |
| Reported 98% with typical use (Manhart et al, 2013) | |||||
Traditional methods
| Traditional Method | Description | How it works | Effectiveness to prevent pregnancy | Comments | |
| Calendar method or rhythm method | Women monitor their pattern of menstrual cycle over 6 months, subtracts 18 from shortest cycle length (estimated 1st fertile day) and subtracts 11 from longest cycle length (estimated last fertile day) | The couple prevents pregnancy by avoiding unprotected vaginal sex during the 1st and last estimated fertile days, by abstaining or using a condom. | 91% with correct and consistent use. | May need to delay or use with caution when using drugs (such as anxiolytics, antidepressants, NSAIDS, or certain antibiotics) which may affect timing of ovulation. | |
| 75% with common use | |||||
| Withdrawal (coitus interruptus) | Man withdraws his penis from his partner’s vagina, and ejaculates outside the vagina, keeping semen away from her external genitalia | Tries to keep sperm out of the woman’s body, preventing fertilization | 96% with correct and consistent use | One of the least effective methods, because proper timing of withdrawal is often difficult to determine, leading to the risk of ejaculating while inside the vagina. | |
| 73% as commonly used (Trussell, 2009) | |||||
What if I am already pregnant?
Well no need to panic at all, Babies indeed are a blessing. Make sure to take good care of yourself and avoid stress. Reproductive Health Uganda clinics are open and you can visit at any working time, Monday- Saturday or better still, call ahead and set yourself an appointment with our well trained doctors.
Our prices are subsidised and are affordable. RHU boosts of over 60 years experience in providing quality and exceptional reproductive health services.

FROM PROTECTING TEETH TO A SAVINGS GROUP
Chunga meno. Swahili for, protect your teeth! In Pajulu Sub County, Arua district, Driwala parish, to be specific is a phrase associated with success. Bizarre, right? True, Chungameno is a name of a saving’s group started by the women vendors of Driwala market. Besides the success harnessed therein, the genesis of this initiative leaves quite the tale.

Women were loosing their teeth to violent Husbands. So they formed a retaliation group to save their teeth! See how this group changed their lives forever!
The charged males would storm the market to grab whatever measly money their wives had made for the day and while at it, beat them up. Or worse, they would wait for them at home, alone, then beat them up to a point that they would lose teeth. A particular group women, about 12, noticed that this was first getting out of hand.
“Women were not settled, there was total chaos!” Harriet Afetia, a leader of the saving’s group, and among the 12 women, narrates. “At least every week, one or two women would have a bruise or lose teeth, it was terrible!” The men wanted to control their money and were frustrated that their wives wouldn’t let them, so they beat them. “We got tired, we decided to do something about it!” Interestingly, it was that decision that started the journey that would later attract a project called prevention plus.

Harriet Afetia, Savings group leader
The story
It was a little over 10 years ago when the women made the decision to take matters into their own hands. See, that afternoon, one of them came to the market bleeding from her mouth and the teeth were just about to come out. She had come to close down her stall and leave the village and her marriage all together. These women gathered together, concerned really, and asked what the issue was this time round. “My husband came back and didn’t find lunch ready, he pounced on me, hit my mouth and left my teeth shaky and gum bleeding,” the woman responded. Puzzled, her fellow women asked, “Lunch, couldn’t he cook it too?”
And just like that, one woman burst out: “We must protect ourselves and protect our teeth!” And these market women, locked in this bitter moment, many of whom didn’t have front teeth, agreed that they would start a group and the name would be, Chungameno! Not two words, but one word. “Chungameno came to arrest the situation!” Afetia exclaims.
But it wasn’t just the violent men that they sought to deal with, even within themselves, they insisted no one better be the perpetuator of violence. They didn’t lay a hand on anyone, but with up to 12 women, matching and chanting towards your home, most men had no alternative but go where the own wanted them to go, a police station. The Sub County leadership was impressed, and they asked police to work with the women.
“As soon we heard that one of us had been beaten, quickly we went as a group and arrested that man,” she recalls. They had become a mob! These women became each other’s keepers, but try as they may, they knew they needed a better strategy, dragging man after man to police was not going to be enough. They were in luck, news of their little group had reached Reproductive Health Uganda (RHU). Soon, their leader, Afetia would be called for a Prevention Plus training, by RHU, a thing they learnt gave their group just the backbone it needed.
Prevention plus impact felt
“During the training, we dealt with the root of all this violence,” Afetia starts. “It was not enough to just keep matching our husbands to police, we needed to find a way to work with them.” Instead of treating the symptom, the Prevention plus training sought to deal with the cause. After sessions of dialogue, training and discussions, she learnt that if money and how money was spent was indeed the cause of most of the bickering, didn’t it make sense to then deal with that issue?
“That training helped me understand this problem properly,” she recalls. The first suggestion was that But first they would need to start a saving’s group! See, while they had been occasionally saving, it was not as comital, and the highest amount many saved was shs500. “I came back also and encouraged the group to first of all start putting more money aside,” she says. The goal was first to make sure no one had all their money on them; so they decided to put the minimum weekly savings at shs2000. They would save all year and only distribute at the end of the year.
But before all of this, they needed to discuss how to include their husbands in this growth. “After distributing the money like this, we always ask these women what they are going to do with the money,” she tells of how the discussion to include men begun. But also, the group attracted the RHU camp; the Prevention Plus team came to offer their services but also preach unity and inclusiveness in families, as opposed to just dealing with the culprits.
Soon, wives begun encouraging their husbands to attend the group meetings and save together. “During these meetings, the people from RHU would come and also teach couples about dangers of violence,” she recalls. This group that started out with just 12 members was now at nearly 200 members, with large number of couples jointly saving and many not even vendors.
Unity and inclusiveness

Rophin Agamile his wife Christine Bako and their family
Rophin Agamile, the area Local Councilor was the first male to join the group, and more than just save, his wife Christine Bako says he has become a better man. Agamile tells of how a session he attended that had guests from South Africa left him a changed man. “I was called as LC1 to welcome the visitors to the Chunagmeno group to talk about Prevention Plus,” he recalls. “These were guests from South Africa who had come to talk to the women’s group, I was impressed by what they said!”
The topic around Father’s Legacy hit a raw nerve. “As a father, what kind of example was I setting?” he remembers asking himself. Agamile used to abuse alcohol, return home in the wee hours to start fights. “When I was around the compound, the children were all quiet!” he narrates regretfully. “As a man, I used not to give chance to my madam to say a word; my words in fact were final in the home.” On a good note, Bako says that man is long gone. “My husband is good to me and my children,” she starts. “Can you believe we save together, we clean and cook food together, and he plays with the children?”
Almost instantly, their little child runs into Agamile’s hands, the peace in their homestead is visible, but is what Afetia said that made this even better. “Rophin is just one example, there are many men who came to save money, but instead became good fathers and husbands,” she says. “We invited the Prevention Plus team to train us on how to keep peace in our homes, and now no single member of our group has lost a tooth since.”

WHEN THE YOUNG PEOPLE MET AND DIALOGUED
It might have been a dump morning that morphed into a drizzly day, but it didn’t define the RHU-organised Inter-University Dialogue that happened over the weekend at Makerere University. Over one thousand students from a host of different institutions around the country thronged the Freedom Square in what would be an intense dialogue into sexuality, culture and religion. (more…)

AFRICAN CITIZENS’ INITIATIVE
ACI goal is to inspire, empower and capacitate our network of volunteers in a peer-to-peer fundraising programme to raise support for health programmes that target women, girls and families in vulnerable, underserved and hard-to-reach communities.

QUALITY SRH INFORMATION AND SERVICES
Reaching most vulnerable and underserved communities with critical SRHR information and services

BECOME A VOLUNTEER
Volunteering can be personally rewarding and helps you give back to your community